By Aarogya Global | Medical Travel Intelligence | May 2026
<p>Nobody expects to find themselves researching hip surgery in another country. Most people start closer to home — a consultation, a referral, a quote — and it is usually at that point that the real journey begins. A waiting list measured in months, not weeks. A cost estimate that is simply not possible. A procedure that is technically available locally but rarely done, by surgeons who see two or three cases a year.</p>
<p>That is where most of the orthopaedic patients who contact us begin. In pain, uncertain, wondering whether what they have heard about Indian hospitals is actually true — or whether it sounds too good to be real.</p>
<p>This piece is for them. And for the referring physicians who want to understand, concretely, what their patients will encounter on the other side.</p>
<hr />
<h2>The Cost Gap Is Structural, Not Superficial</h2>
<p>A total hip replacement in the United States costs between $30,000 and $50,000. A private procedure in the United Kingdom runs between £15,000 and £25,000, and that figure assumes no complications and no extended physiotherapy. In India, the same surgery — performed by surgeons using the same imported implants, in JCI-accredited facilities — costs between $5,000 and $8,000, all-inclusive. That covers the procedure, the implant, the hospital stay, physiotherapy, and post-operative care.</p>
<p>For patients in Nigeria, Kenya, Tanzania, Ethiopia, or across the Gulf who are paying entirely out of pocket, this difference is not marginal. It is the difference between treatment and no treatment.</p>
<p>The savings are structural. India’s healthcare economics such as lower cost of living, high surgical volumes, a deep domestic pool of specialist talent produce a pricing gap that Western systems cannot close. This is not a compromise. It is a different system, operating at a different scale, with outcomes that speak for themselves.</p>
<hr />
<h2>What JCI Accreditation Actually Means for an Orthopaedic Patient</h2>
<p>The hospitals Aarogya Global partners with carry JCI accreditation – the same international certification body that audits leading hospitals in the United States and Europe. For an orthopaedic patient, this is not a formality. It has direct clinical implications.</p>
<p>JCI-accredited hospitals operate under mandatory patient identification protocols before every procedure — surgery, medication, anaesthesia. They maintain documented infection control standards. Their surgical teams work within quality review frameworks that require regular outcome reporting and complication tracking. These are not aspirational standards. They are audited, and hospitals that fall short lose the certification.</p>
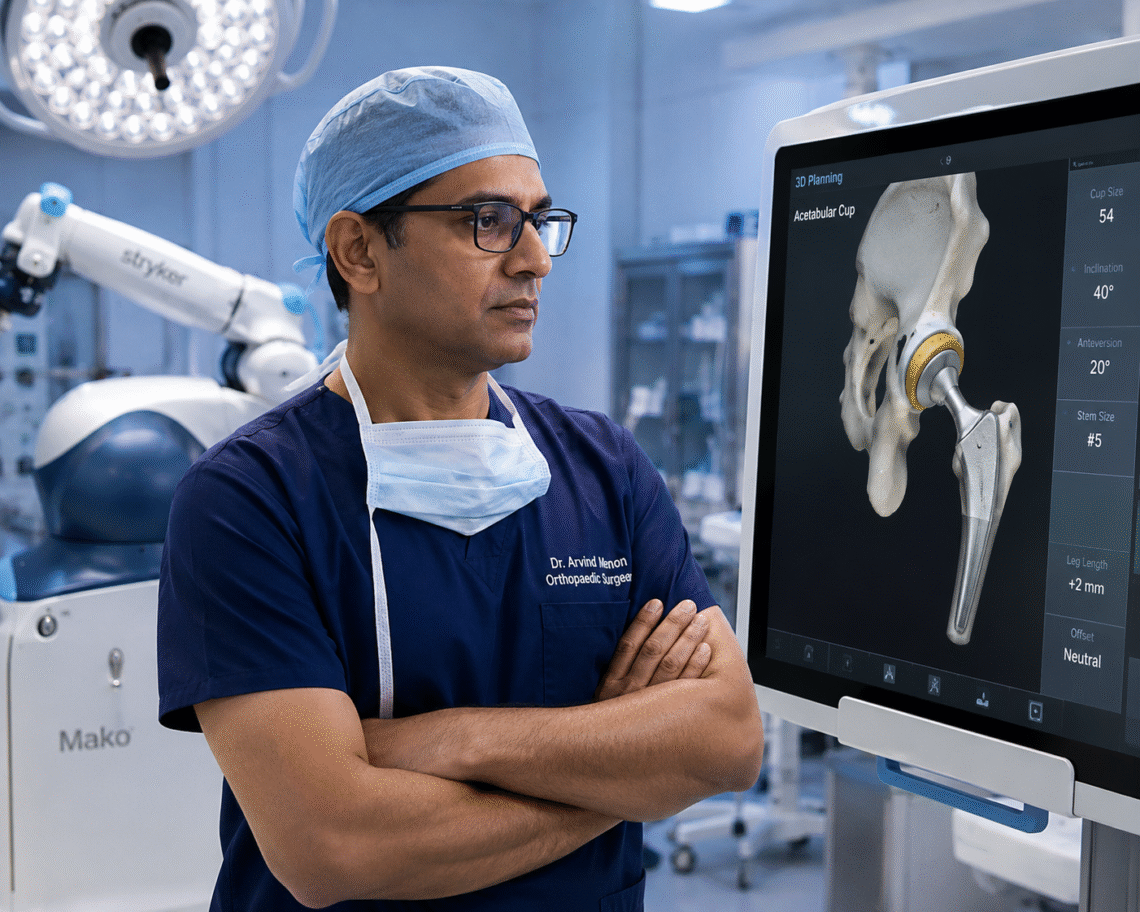
<p>Institutions like Apollo Hospitals, Fortis Healthcare, Manipal Hospitals, Medanta, and Kokilaben Dhirubhai Ambani Hospital operate robotic surgery suites for hip and knee replacements — the same Stryker Mako and Zimmer Biomet platforms used in New York and London. Implant positioning accuracy within one to two degrees. Infection rates that sit alongside, not beneath, the benchmarks of top-ranked American centres.</p>
<p>The technology is not an approximation of what exists elsewhere. It is the same technology, in the hands of surgeons who use it every week.</p>
<hr />
<h2>Surgical Volume and What It Means in Practice</h2>
<p>Volume matters in orthopaedic surgery more than in almost any other specialty. An orthopaedic surgeon in the United States might perform 150 to 200 hip replacements per year. Their counterpart at a large Indian tertiary hospital routinely performs 400 to 600. That repetition is not incidental to quality — it is the mechanism through which quality is built.</p>
<p>India’s leading orthopaedic surgeons hold fellowships from the Royal College of Surgeons, the American Academy of Orthopaedic Surgeons, and other internationally recognised bodies. Many trained in the UK, the US, or Germany before returning to practice in India. They publish in journals like The Bone and Joint Journal. They present at international conferences. And then they go back to operating lists that give them a level of procedural experience that simply cannot be replicated in lower-volume settings.</p>
<p>For a patient about to have a hip replaced, the person holding the instruments matters enormously. Volume is how surgeons become the kind of person you want holding them.</p>
<hr />
<h2>From Chronic Pain to Walking Assisted: What the Timeline Looks Like</h2>
<p>In the NHS, the current wait for a hip replacement can stretch to twelve to eighteen months from referral. That is twelve to eighteen months of worsening pain, reduced mobility, interrupted sleep, and a steady decline in quality of life. For a patient in their fifties or early sixties — still working, still raising a family — this is not a minor inconvenience. It is a significant loss.</p>
<p>In India, the process from first contact to discharge typically spans seven to fourteen days. Pre-surgical assessments, imaging, and anaesthesia consultations are completed within the first forty-eight hours. Surgery follows. Physiotherapy — and this surprises most patients — begins within twenty-four hours of the procedure.</p>
<p>By day three or four, the majority of hip replacement patients are walking assisted laps of the ward corridor. They are not passive. They are already in recovery.</p>
<p>Before discharge, patients receive a written rehabilitation plan that covers every medication, wound care instruction, physiotherapy milestone, and follow-up date. Their surgeon’s operative report and discharge summary are sent electronically to their physician at home, so that continuity of care does not depend on the patient carrying a folder of paper documents through an airport. The handover is built into the process, not left to chance.</p>
<hr />
<h2>Why India Specifically Dominates Hip Replacement</h2>
<p>Hip replacement is not an undifferentiated surgical market. Outcomes depend on implant selection, surgical approach, intraoperative precision, and early rehabilitation — and India’s leading centres have invested systematically in each of these.</p>
<p>Implants from Zimmer Biomet, Stryker, and DePuy — the same manufacturers supplying American and European hospitals — are available in India at significantly lower markups than in Western markets. The Mako robotic system, which improves cup positioning accuracy and has been associated with reduced revision rates, is widely available at top-tier centres. The anterior approach to hip replacement — less muscle disruption, faster recovery, earlier weight-bearing — is practised routinely rather than offered as a specialist upgrade.</p>
<p>Physiotherapy begins early. Discharge is planned, not reactive. And the all-inclusive pricing model — surgery, implant, hospital stay, rehabilitation — means there are no billing surprises waiting on the other side of the procedure. Patients and families know the number before they board the plane.</p>
<p>Most international patients receive an e-Medical visa within seventy-two hours. India is the world’s second-largest English-speaking nation. The practical barriers to travel are lower than most patients expect.</p>
<hr />
<h2>Three Patients. Three Different Starting Points. One Pattern.</h2>
<p><strong>Grace, from Lagos</strong></p>
<p>Grace is 58. She had been managing severe osteoarthritis in her right hip for nearly two years — cortisone injections, walking aids, progressively less sleep — when her orthopaedic consultant in Nigeria recommended a total replacement. The cost of the procedure at a private hospital in Lagos was beyond what her family could arrange. She contacted Aarogya Global after seeing a referral from a colleague of her doctor.</p>
<p>Twelve days after that first contact, she was admitted to a JCI hospital in Chennai. Her surgeon had trained in the UK and had performed over four hundred hip replacements in the previous year alone. By day four post-surgery she was walking the ward corridor with a frame. She flew home on day ten. Her physiotherapist in Lagos received her rehabilitation protocol the day before she landed. Six weeks later, her consultant described her recovery as ahead of schedule.</p>
<p>She told her Aarogya Global coordinator: <em>I had no idea what to expect. I arrived nervous. I left feeling like I had been given something back.</em></p>
<p><strong>James, from Nairobi</strong></p>
<p>James is 64. His cardiologist had cleared him for elective surgery, but the quotes he received for hip replacement — both in Kenya and from a facility in South Africa — were not manageable. His daughter, who works in healthcare administration in the UK, had heard about Aarogya Global through a professional contact.</p>
<p>We reviewed his records within forty-eight hours. A surgeon in Hyderabad confirmed he was a suitable candidate. The all-in cost was less than a third of the South Africa quote. He travelled with his wife. The procedure was robotic-assisted. He was discharged on day eight. His cardiologist in Nairobi had the operative report before James’s return flight landed.</p>
<p><strong>Hana, from Addis Ababa</strong></p>
<p>Hana is 51 and had been on a waiting list at a public facility in Ethiopia for nearly a year when her daughter helped her submit her records to us. The hip deterioration had progressed to the point where her local physician was concerned about avascular necrosis. Speed mattered.</p>
<p>We placed her with a surgeon in Delhi within a week of receiving her imaging. Her visa was processed in sixty hours. She had surgery fourteen days after her first contact with Aarogya Global. She told us afterwards: <em>I had been waiting so long I had started to accept that this was just my life now. I did not expect it to move this fast.</em></p>
<hr />
<h2>What Aarogya Global Does — And Why the Distinction Matters</h2>
<p>We are sometimes described as a medical tourism company. That is technically accurate and somehow also misses the point entirely.</p>
<p>What we do is connect medical communities. The orthopaedic surgeon in Nairobi who knows his patient needs a procedure she cannot access locally at a price she can manage. The referring physician in Lagos who wants his patient seen by a specialist who does this every day, not three times a year. The family in Addis Ababa who has found contradictory information online and does not know what to trust.</p>
<p>We sit between those worlds. Every patient who comes to us receives a clinical review before any travel is recommended. We identify the right institution and the right surgeon for that specific diagnosis — and we only recommend travel once we are confident the match is correct. We do not send people to India and see what happens when they land.</p>
<p>We maintain active communication between the treating hospital in India and the referring physician at home throughout the patient’s journey. Discharge summaries, operative reports, rehabilitation protocols — these do not stay in India. They travel home with the patient, into the hands of the physician who will continue their care.</p>
<p>And we do not operate on referral commission structures that reward volume over clinical appropriateness. If India is not the right option for a patient, we will say so. Our value to the physicians who refer patients to us depends entirely on that integrity. It is not a small thing.</p>
<hr />
<h2>A Final Word</h2>
<p>Orthopaedic disease — hip degeneration, knee failure, spinal deterioration — does not wait. It compounds. Every month of delayed treatment is a month of worsening function, increasing pain, and narrowing options. The patients who reach us having already waited twelve or eighteen months almost always say some version of the same thing: <em>I wish I had done this sooner.</em></p>
<p>India’s leading orthopaedic centres offer something rare: genuine surgical excellence, at a cost that is accessible to the patients who need it most, without the waiting that makes delay a foregone conclusion in many health systems. That combination does not exist in many places in the world. It exists here.</p>
<p>If you want to understand whether this is the right option for you or for a patient you are referring, we are here. No obligation. Just a conversation.</p>
<hr />
<p><em>Aarogya Global partners with JCI and NABH accredited hospitals across India to facilitate medical travel for international patients from Africa and the Middle East. Upload your reports and book a free consultation at <a href=”https://aarogyaglobal.com”>aarogyaglobal.com</a>.</em></p>
<p><em>Cite as: Aarogya Global. (2026). “Why India Has Become the World’s Most Trusted Destination for Orthopaedic Care.” Aarogya Global Medical Travel Intelligence.</em></p>




